| |
Oral Drugs for Benign Prostatic Hyperplasia
|
 |
Benign prostatic hyperplasia
|
| |
|
|
Benign prostatic hyperplasia (benign prostatic hypertrophy) (BPH) is a noncancerous (benign) enlargement of the prostate gland that can make urination difficult. An enlarged prostate is common in men after the age of about 50. About 4 out of every 10 men over the age of 50 (40 per cent) and 3 out of 4 men in their 70s (75 per cent) have urinary symptoms that are caused by an enlarged prostate.
|
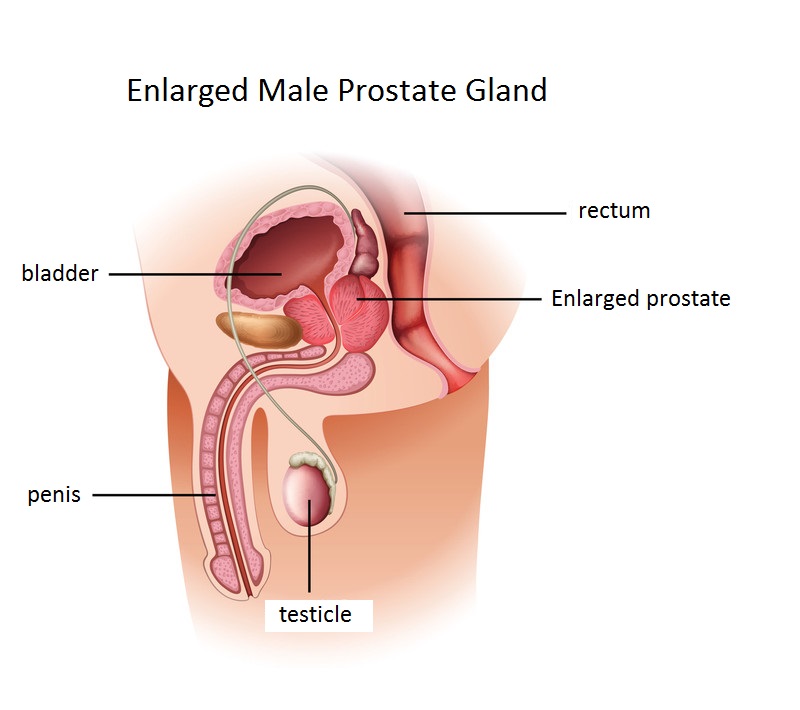
Prostate gland lies just beneath the bladder, and is normally about the size of a walnut/golf ball. The prostate goes through two main growth periods as a man ages. The first occurs early in puberty, when the prostate doubles in size. The second phase of growth begins around age 25 and continues during most of a man’s life. Benign prostatic hyperplasia often occurs with the second growth phase.
|
The prostate is a small gland that only found in men, it produces the fluid that carries sperm during ejaculation. The gland surrounds the urethra at the neck of the bladder. The bladder neck is the area where the urethra joins the bladder. The bladder and urethra are parts of the lower urinary tract. The urethra is the tube that carries urine from the bladder to the outside of the body.
|
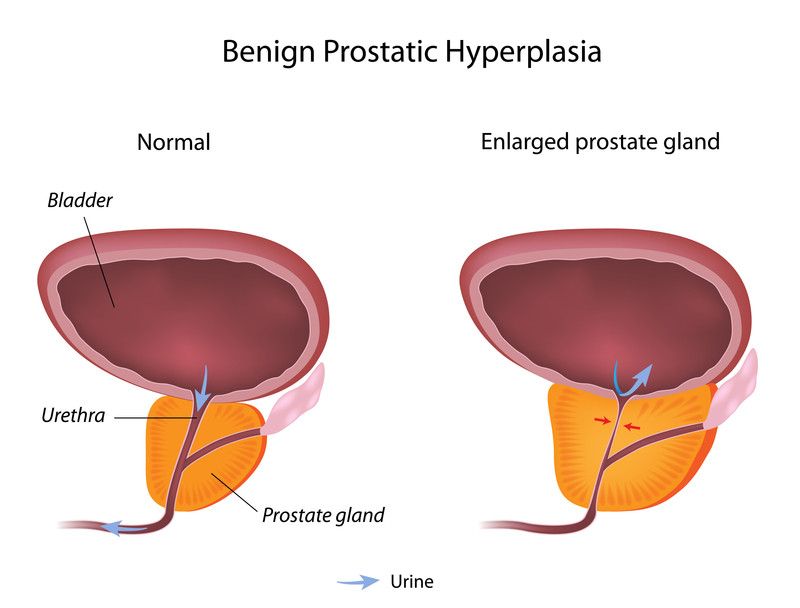
Urethra passes through the center of the prostate, as the prostate enlarges, the gland presses against and pinches the urethra. As the bladder overworked from trying to pass urine through the blockage, the bladder wall becomes thicker. Eventually, the bladder may weaken and lose the ability to empty completely, leaving some urine in the bladder even after urination. The narrowing of the urethra (slow down the flow of urine) and urinary retention (inability to empty the bladder completely) accounts for many of the problems associated with benign prostatic hyperplasia.
Lower urinary tract symptoms (LUTS) is a term used to describe a range of symptoms related to problems of the lower urinary tract (bladder, prostate and urethra). LUTS can be caused by prostate enlargement or other conditions. They are best categorized into voiding, storage or post-micturition symptoms to help define the source of the problem.
|
|
- Voiding symptoms include weak or intermittent urinary stream, straining, hesitancy (may have to wait at the toilet for a while before urine starts to flow, terminal dribbling (towards the end of passing urine, the flow becomes a slow dribble) and incomplete emptying (have a feeling of not quite emptying your bladder).
- Storage symptoms include urgency, frequency, urgency incontinence and nocturia (urination at night).
- The major post-micturition symptom is post-micturition dribbling, which is common and bothersome.
|
|
▲ back to top
Treatment |
|

|
Consideration for treatments usually depended on how severe and bothersome the symptoms are. To choose the best option, your doctor will consider your symptoms, the size of your prostate, any complications from BPH, other health conditions you might have and your preferences. There are three main types of treatment for BPH:
|
- Watchful waiting (monitoring without active intervention)
- Drug treatment
- Surgery
|
Watchful waiting is suitable for men with mild to moderate symptoms that are not bothersome, and for some men with moderate to severe LUTS who have not yet developed complications of LUTS and bladder outlet obstruction (BOO) (e.g. renal insufficiency, urinary retention or recurrent infection). The patient is monitored and advised on lifestyle measures that may improve symptoms; these include decreasing fluid intake at specific times such as bedtime or when going out, reducing caffeine and alcohol intake in general, avoiding antihistamines and decongestants and bladder re-training techniques.
|
Drug treatment is used if lifestyle changes (watchful waiting) are not enough to improve the quality of life. It is important to let your doctor know about any medicines or herbal remedies you are already taking or will take, in case they interfere with the medicines for an enlarged prostate.
|
|
Your doctor may recommend surgery if lifestyle changes or medicines do not control your symptoms. Untreated, prostate gland enlargement can block the flow of urine out of the bladder and cause bladder, urinary tract or kidney problems.
|
|
|
▲ back to top
Oral drugs for benign prostatic hyperplasia
|
|
 |
Medications used in benign prostatic hyperplasia include:
|
1. Alpha blockers (e.g. alfuzosin, doxazosin, tamsulosin or terazosin).
These drugs act on the smooth muscle tone within the prostate and the bladder neck which decreases urethral resistance and allows the urethra
to get bigger and so makes it easier to pass urine. These drugs can produce symptomatic relief within weeks. They are given to men with moderate to severe LUTS.
|
2. 5-alpha reductase inhibitors (e.g. finasteride and dutasteride).
These drugs inhibit the enzyme 5-alpha reductase which converts testosterone to dihydrotesterone (DHT), DHT is the primary androgen involved in normal and abnormal prostate growth. Through this inhibition, production of DHT is reduced hence prostate size is decreased. 5-alpha reductase inhibitor reduces the risk of progression to urinary retention and prostatic surgery, and are given particularly to men with urinary symptoms, large prostates, who are considered to be at high risk of progression (for example, older men). Response of 5-alpha reductase inhibitors may be delayed and treatment may be required for 6 months or more to assess whether benefit has been achieved.
|
Combination of an alpha blocker and a 5-alpha reductase inhibitor is also used for treatment. This combination treatment is considered suitable for patients with LUTS associated with demonstrable prostatic enlargement who are at significant risk of progression. There is combination product of 5-alpha reductase inhibitor and alpha blocker (dutasteride and tamsulosin) registered.
|
|
All the above named medications are registered in Hong Kong and are available in oral dosage form. They are prescription only medicine and must be administered strictly under doctor’s instruction.
|
|
▲ back to top
Common side effects and precautions
|
Drugs for BPH
|
Common side effects
|
Precautions
|
|
Alpha blockers
|
| |
Alpha blockers
(e.g. alfuzosin, doxazosin, tamsulosin or terazosin)
|
- drowsiness, hypotension (notably postural hypotension), syncope (faint), asthenia (weakness), dizziness
- headache
- blurred vision, intra-operative floppy iris syndrome (most strongly associated with tamsulosin)
- dry mouth, rhinitis (inflammation of the lining of the nose)
- tachycardia, palpitations (rapid or irregular heart beat)
- gastro-intestinal disturbances
- oedema
- depression
- erectile disorders (including priapism (persistent painful erection of the penis))
|
- Since alpha 1-selective alpha blockers reduce blood pressure, patients receiving antihypertensive treatment may require reduced dosage.
- Alpha-blockers should be avoided in patients with a history of postural hypotension and micturition syncope.
- Caution is required in the elderly and in patients undergoing cataract surgery (risk of intra-operative floppy iris syndrome).
- Should always tell your doctor if you are taking or have recently taken any other medicine, because they might interact with alpha blockers.
- Especially important to tell your doctor if you are taking other medicines to treat high blood pressure or erectile dysfunction.
- This drug may affect your ability to drive or operate machinery safely, particularly when you first start to take them. They may make you feel weak or dizzy. If affected, do not drive or operate machinery and contact your doctor immediately.
- Do not use in patient with sever hepatic impairment (alfuzosin, doxazosin, tamsulosin and terazosin), use with caution in patient with mild to moderate hepatic insufficiency, dose adjustment may be required for alfuzosin and doxazosin.
- Dose adjustment is required for mild to moderate renal insufficiency (alfuzosin, doxazosin), use tamsulosin with caution in severely renal impaired patients (creatinine clearance of less than 10 ml/min).
- Use alfuzosin with caution in patient with acute heart failure; history of QT-interval prolongation; concomitant use with other drugs known to prolong QT interval. Discontinue if angina worsens.
|
|
5-alpha reductase inhibitors
|
| |
5-alpha reductase inhibitors
(e.g. finasteride and dutasteride)
|
- impotence (not able to achieve or maintain an erection), decreased libido, ejaculation disorders
- breast tenderness and enlargement
| |
For finasteride the following also reported:
|
- testicular pain
- hypersensitivity reactions (including lip and face swelling, pruritus and rash)
- male breast cancer
|
- Dutasteride and finasteride affects a blood test for prostate-specific antigen (PSA) which is sometimes used to detect prostate cancer (decrease serum concentration of prostate cancer markers such as PSA).
- Both dutasteride and finasteride are excreted in semen and use of a condom is recommended if sexual partner is pregnant or likely to become pregnant.
- Cases of male breast cancer have been reported. Any changes in breast tissue such as lumps, pain, or nipple discharge should report to the doctor promptly.
- Both dutasteride and finasteride may increase risk of high-grade prostate cancer.
- Avoid to use dutasteride in severe hepatic impairment. Use with caution in patients with mild to moderate hepatic impairment.
- Use finasteride with caution in patients with liver function abnormalities.
- Dutasteride is absorbed through the skin, therefore, women, children and adolescents must avoid contact with the drug.
- Patients on dutasteride should not donate blood until 6 months after their last dose. The purpose of this deferred period is to prevent administration of dutasteride to a pregnant female transfusion recipient.
|
|
|
▲ back to top
General advice
|
|
 |
-
Avoid drinking any liquids for one to two hours before going to bed - this will reduce your chances of waking up during the night to pass urine (nocturia).
- Emptying your bladder - go to the toilet before long journeys or when you know you will not be able to reach a toilet easily.
- Double voiding - this involves waiting a few moments after you have finished passing urine before trying to go again. It can help you to empty your bladder properly.
- Stop drinking alcohol and caffeine, or limit your consumption of them - they can irritate your bladder and make your symptom worse.
|
- Bladder retraining - there are some techniques that can help you to hold on for longer before going to the toilet. Ask your doctor for more information.
- Eating more fruit and fiber - This will help you to avoid getting constipation, which can put pressure on the bladder.
- Exercise regularly - research has shown that moderate exercise, such as walking for 30 to 60 minutes a day, can improve symptoms.
|
|
▲ back to top
Communication with your doctor
|
|
 |
|
- Drugs for benign prostatic hyperplasia (BPH) should be used under medical supervision.
- Check with your doctor whether any medicines you take may be making your urinary symptoms worse, such as anti-depressants or cough and cold medicines (may contains decongestants, caffeine and / or antihistamine).
- If you notice changes in your urinary habits, visit your doctor in the first instance. It is very important that you tell your doctor if you are taking any kind of herbal or complementary medicine.
|
- Seek medical advice as soon as possible if you experience any symptoms or side effects suspected to be related to your BPH drugs. Your doctor may review your medications.
- Inform your doctor if the BPH drugs do not work. It may be related to some underlying diseases.
|
|
▲ back to top
Storage of oral drugs for benign prostatic hyperplasia |
|
Oral drugs for benign prostatic hyperplasia should be stored according to condition specified on the label, usually kept in a cool and dry place. Furthermore, drugs should be kept properly in places unreachable by children to prevent accidental ingestion.
|
|
▲ back to top
|
|
Acknowledgement: The Drug Office would like to thank the Professional Development and Quality Assurance (PD&QA) for their valuable contribution to the preparation of this article.
|
|
|
|
|

